The Fitness Zone

Don’t fear the disc bulge! Banishing low back pain
Low back pain is not forever, but fitness and strength training is! Physiotherapist and strength rehab coach Dr Andrew Lock explores how to assess and address a client’s back pain.
The definition of insanity has been presented as ‘doing the same thing and expecting a different outcome’. This is the essence of most people who experience low back problems. Symptoms are often treated by a health professional such as a physiotherapist, chiropractor, osteopath or myotherapist but the cause is not addressed. This is where you, as a fitness industry professional, can make a huge impact.
Health and fitness are the cornerstones to breaking the back pain cycle. Changing the factors that create low back injury are the key to freedom and progress. Personal trainers and health professionals must understand movement, posture, and exercise technique – the major influences upon recurrent low back issues.
“Changing the factors that create low back injury are the key to freedom and progress”
Rest changes nothing

If you have ever had a flat tyre on your car, you will have noticed that leaving it out the front of your house overnight doesn’t help fix the tyre. When you wake up, the car will still have a flat tyre. If you do nothing, you change nothing.
To change your clients’ lives, do something, something different!
Where to start when understanding a low back problem? Let us begin with a simple acronym that will help you assess and change a client’s episodic low back pain (and, in fact, any joint pain). The three letters you need to remember are P A M:
P is for PASSIVE
Passive tissues are those that you cannot contract, the non-contractile tissue, i.e. bones, ligaments, discs.
A is for ACTIVE
Active tissues are those that you can contract, i.e. muscles.
M is for MOVEMENT
Movement patterns are the way we use the Active and the Passive tissues to live and lift.
In low backs, most injury occurs when a poor movement pattern (M) occurs, or is repeated, that involves a weak muscle/group (A), and the passive tissue (P) is loaded to a point where it fails and injury results.
Understanding this relationship is the key to training a client who has experienced, or has a history of, low back problems.
We need to:
- address and correct poor movement patterns
- strengthen weak muscle groups
- understand and consider daily work/life postures
Do you need to know what has been injured?

Often, I ask a client “What is your problem?” and they will answer “I have a disc bulge at…”. I immediately stop the client and say, “I didn’t ask you what your diagnosis is, I asked you what your problem is. What are you having trouble doing that you are seeking my assistance with?”
The client’s answer will help define the true problem.
Interestingly, you do not need to know the specific tissue that has been injured. What you do need to know is what movement or posture produces the pain. We call this the ‘biomechanical trigger’.
Solving the problem of the biomechanical trigger gives us our training plan.
With further education you can learn which tissue or structure is the source of the pain, which is useful when explaining the rationale for your exercise and programming choices to your client. I teach the science of anatomy and biomechanics for this in my courses. Remember: it’s more important to know the movement triggers than it is the actual structure.
“The most common problems we encounter are flexion intolerances”
Understanding directional assessment
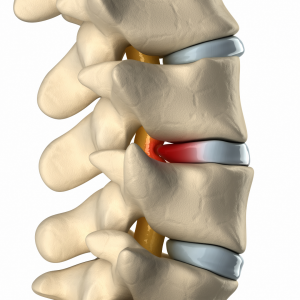
The two most common triggers involve directions of movement. Clients will tend to be flexion or extension intolerant. For example, a fast bowler who has back pain may be extension intolerant when they lean back to deliver the ball, as this is lumbar extension. A bodybuilder, meanwhile, may have back pain at the bottom stage of the squat when they ‘butt wink’, due to lumbar flexion.
Once we understand this, we can examine other related factors. The most common problems we encounter are flexion intolerances: these are often in those who come to us with a disc bulge diagnosis. Aggravating postures and movements that are consistent with this presentation include problems with bending forwards, tying shoes and an intolerance of longer sitting periods.
Discussing the aggravating factors with your client will tend to give you the answers you need to be aware of when creating a training program that a client can tolerate.
The solution must be specific
Remember our car trouble? Do not bother looking under the hood when the problem is a flat tyre. Your training programs for low back problem clients must be specific, not general.
This requires us to adhere to the SAID principle: Specific Adaptation to Imposed Demand.
“If a problem has a movement direction issue, then it is time to correct the movement pattern”
Addressing the movement
If a problem has a movement direction issue, then it is time to correct the movement pattern. How your client moves into that direction will need to be addressed in the program. The most common problem in ongoing low back issues is knowing the difference between flexion moment (in which muscles are activated, regardless of any movement occurring) and flexion movement (bending like a fishing rod). Even most physiotherapists I have spoken to do not know this simple but important distinction. Essentially, we find the trigger is often due to poor hip contribution to bending forward: the person uses their lumbar flexion too early, has muscle weakness in holding a neutral spine and at the painful segment there is flexion stress. These are areas that a competent fitness trainer can address!
Defining strength
Strength is a skill, it’s not just muscle size. Skill is created by practice, perfect practice at that. To change a movement pattern is to create strength in that pattern.
Consider two parts to the strength definition (referring back to the PAM acronym). Firstly, improving the skill in a movement pattern (M); and secondly, hypertrophy an undeveloped muscle group (A).
1. Movement patterns
I use the strength sciences to produce the most successful low back training outcomes, no matter the size of the disc injury. Teaching movement pattern correction is imperative, for example, a hip hinge pattern that is glute dominant in spinal neutral, rather than a spinal flexion lumbar dominant pattern that triggers the problem. This requires an increase in glute contributions to movement patterns.
“People who have long term chronic low back problems will have atrophied multifidus”
2. Hypertrophy
After low back injury, the multifidus muscle, which is the deepest spinal erector, has been shown to atrophy. It is an important part of the spinal segmental control system.
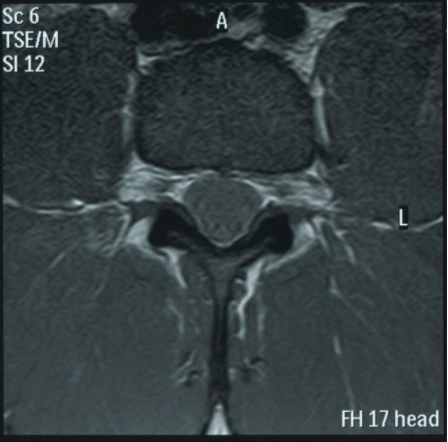
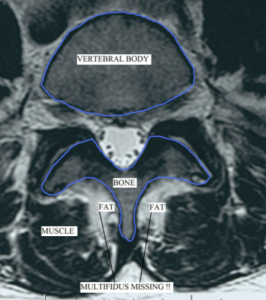
Research clearly demonstrates that people who have long term chronic low back problems will have atrophied multifidus and will continue to do so until a specific strength retraining program is undertaken. That means, until corrected they will have a greater likelihood of recurrent episodic problems and continue to function less than optimally. It does not get better with rest!
Research also shows that a person who has had even one episode would have reduced multifidus function in the future. Every person who has had even one episode of low back pain should have multifidus hypertrophy and timing rehabilitation assessed. It should be done in an integrated whole body stability program. This is where a fitness professional can safely and appropriately implement a strength training routine.
The BASE 5
I created the BASE 5 exercises as the beginning to a lumbar spine-specific training program. These five exercises form the base of the low back training pyramid. The BASE 5 has two glute and three core strengthening exercises in an extremely specific order. From this base, I have produced a series of over 100 progressions and regressions that address each component, can move in any direction and can be programmed to restore a pain-free and safe conventional deadlifting and squat performance.
The BASE 5 are:
- Lock Clam 25 reps each side 2 sets
- Perfect Front Plank 30 seconds 2 sets
- Side Plank 15 seconds each side 2 sets
- Shoulder Taps 10 reps each side 2 sets
- Prone Hip Extension 10 reps each side 3 sets
This is done twice per day and always prior to any training. The instructional for this can be found on my Instagram page @andrew_lock_strength
Dr Andrew Lock, PhD
Andrew is a physiotherapist, education provider and the strength rehabilitation professional to many international athletes and their coaches. Through his business United Health Education, he delivers face-to-face glute training workshops with Dr Dani Antonellos. He also presents on the three power lifts with strength coach Sebastian Oreb via Strength System, and shares details of his Low Back Courses via his Instagram page.
unitedhealthed.com/collections/workshops / strengthsystem.com / instagram.com/andrew_lock_strength

Read more articles
Disclaimer: Where Certificate III in Fitness, Cert III/Cert 3, or Fitness Coach is mentioned, it refers to SIS30321 Certificate III in Fitness. Where Certificate IV in Fitness, Cert IV/Cert 4, or Personal Trainer is mentioned, it refers to SIS40221 Certificate IV in Fitness. Where Master Trainer Program™ is mentioned, it refers to Fitness Essentials and SIS40221 Certificate IV in Fitness. Where Master Trainer Plus+ Program™ is mentioned, it refers to SIS30321 Certificate III in Fitness and SIS40221 Certificate IV in Fitness. Where Certificate IV in Massage or Cert IV/Cert 4 is mentioned, it refers to HLT42021 Certificate IV in Massage Therapy. Where Diploma of Remedial Massage is mentioned, it refers to HLT52021 Diploma of Remedial Massage.









Ready to kickstart your fitness career? Speak with our friendly Careers Team on 1300 669 669 or enquire now online.
Enquire Now eCampus Login IGNITE Learning Platform Login